Mental health disorders have emerged as a potentially significant factor in workers' compensation. This article focuses on potential impacts that post-traumatic stress disorder (PTSD), a mental health condition that some people develop after they experience a shocking, scary, or dangerous event, may have on WC system costs.
In recent years, there has been an increase in legislative activity across the country to broaden or establish eligibility for WC benefits for PTSD. The momentum of such measures has grown, and could be accelerated somewhat, given the spotlight the COVID-19 pandemic has cast on the potential for workers to contract PTSD from their employment—particularly in the healthcare field. In this paper, we review examples of WC benefit eligibility criteria for PTSD, available data and the potential impact of PTSD on overall WC costs, including possible effects stemming from the pandemic and other stressors.
How Do WC Benefit Eligibility Criteria for PTSD Vary by State?
There is much variation in WC benefit eligibility requirements for PTSD between states. The first question we reviewed is whether PTSD—without a corresponding physical injury—is explicitly addressed as being a compensable injury or occupational disease under WC statutes.
- Statutes may generally address WC for a mental injury or illness in a variety of ways, explicitly exclude mental injuries not accompanied by physical injuries (a mental injury or disability that arises without a physical injury is also known as a “mental-mental” injury) or limit mental-mental injuries to certain situations such as crimes of violence.
- If PTSD is compensable as a covered injury or occupational disease under a state’s WC statutes, it may be compensable for all occupations or only for some subset of occupations such as “first responders” (e.g., law enforcement officers, firefighters and emergency medical technicians).
- In the case of first responders, statutes typically reference the PTSD subset of mental injuries.
If a state provides WC benefits for PTSD without a physical injury, what conditions need to be satisfied for it to be a compensable claim?
- Must the condition result from a specific incident, or can it arise over time as a result of cumulative exposure to several events? (When the condition is brought about by repeated traumatic events, it may also be referred to as continuous traumatic stress disorder, or CTSD.)
- Must the nature of the traumatic event preceding the PTSD be extraordinary in relation to the average worker’s job experiences, or in relation to other employees in the same occupation?
- What is the burden of proof required to establish eligibility for WC benefits? For example, must PTSD be proven with clear and convincing evidence or with a preponderance of evidence? Is PTSD associated with a presumption that it arose out of and in the course and scope of employment?
- What type of healthcare professional may make the diagnosis, and what standards can they use?
Some states have legislative proposals that consider establishing or expanding eligibility for WC benefits resulting from PTSD to first responders or a broader group of occupations. Some others have considered increasing coverage to all occupations under certain conditions. Several states where mental injuries may already be eligible for WC benefits have introduced legislation to provide a presumption that PTSD in first responders occurred in the course of employment.
In jurisdictions where NCCI provides ratemaking services, first responder classes only account for approximately 1.6% of privately insured costs, with most states ranging from 0.5% to 3.0%. Therefore, legislation focusing on first responders may have a relatively small impact on overall privately insured WC costs. But it may have a significant impact for the affected classifications. On the other hand, legislation affecting all classes could have a significant statewide impact.
What WC Data Is Available on PTSD?
WC data on PTSD is limited due to both the relative scarcity of PTSD claim data, in general, and limited data reporting for first responder employer groups. If legislation is enacted making PTSD more readily compensable under WC, the subsequently reported additional data could be used in future PTSD cost impact analyses. Until a significant volume of credible WC PTSD data becomes available, non-WC data may be leveraged.
What Are the Incidence Rates of PTSD?
We can get a general idea of PTSD frequency in the workplace by analyzing incidence rates from published PTSD studies and meta-studies of the general population, first responders, veterans and those in other occupations.
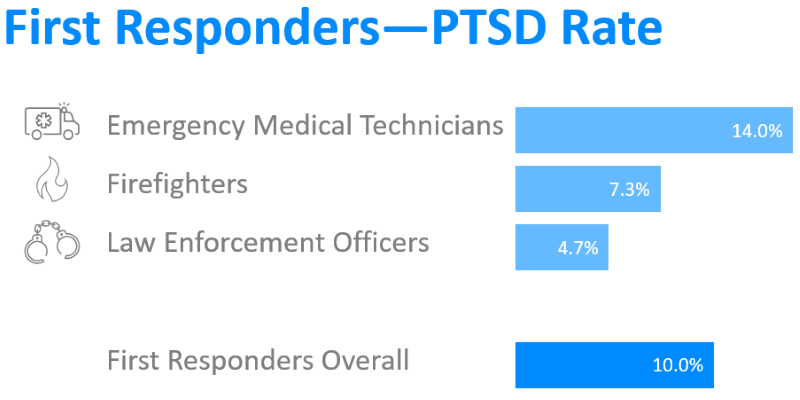
For the general population, a 2016 epidemiological study indicated that 6.1% of American adults experienced PTSD in their lifetime, while 4.7% had it as a condition during the most recent year. The presence of PTSD in the “most recent” year does not indicate when the event or events occurred that led to the condition. So, care must be taken if these prevalence rates are extrapolated to estimate annual WC claim frequency, which is the likelihood that a worker will file a PTSD claim in a particular year and that the claim is accepted.
See also: Workers Comp Trends for Technology in 2021
There have been numerous PTSD studies on first responders. One worldwide meta-analysis estimates a 10% average PTSD rate for first responders overall, where the average rates vary by occupation.
Care is needed when comparing the results of studies that were conducted in varying locations and time periods, and that use differing methods to identify and analyze the incidence of PTSD. Further, it is possible that reported mental illness from traumatic events in the workplace may be increasing relative to levels reflected in past studies.
What About the COVID-19 Pandemic?
While some employees have been working from home, many employees classified as “essential workers” have continued to work at their usual place of employment. This latter group may have faced a higher risk of contracting COVID-19 and possibly experienced more fears and anxiety about becoming infected themselves or infecting their loved ones. In particular, early data suggests that first responders and healthcare workers may have been disproportionately affected by COVID-19—accounting for almost 75% of all COVID-19 claims reported to NCCI as of year-end 2020. Some of these workers have provided direct care to people with the virus, often in overburdened areas. As a result, they may experience significant physical and psychological strain. For example, a sample of 571 frontline workers in the Rocky Mountain region surveyed between April and May 2020 showed 15% to 30% reported traumatic stress.
The myriad of issues faced by first responders and those on the front lines of the pandemic have been well-documented. For example, one writer opines: “Over the last year, there has been the psychological trauma of overworked intensive care doctors forced to ration care, the crushing sense of guilt for nurses who unknowingly infected patients or family members and the struggles of medical personnel who survived COVID-19 but are still hobbled by the fatigue and brain fog that hamper their ability to work.” Extended periods of stressful conditions resulting from the COVID-19 pandemic could mean that these workers may suffer trauma not necessarily from a specific extraordinary event, but perhaps from continuous stress.
Mental health was reported as a significant concern for healthcare workers before the COVID-19 pandemic, and COVID-19 appears to have increased the stress, with 37% reporting “mental health issues” in 2019 versus 41% in 2020. And 58% of healthcare workers say mental health issues have affected their work more since the COVID-19 pandemic began. If any resulting emotional impact persists, it could increase the prevalence of PTSD and CTSD among healthcare workers after the pandemic.
Some other workers, such as nursing home staff, have also disproportionately suffered from COVID-19-related stress. One survey taken between May and June 2020 revealed some of the same adverse conditions for these workers as noted above for healthcare workers.
At this writing, it remains to be seen how COVID-19 will affect the propensity to file PTSD claims in those states that have chosen or will choose to make PTSD or other mental-mental claims eligible for WC benefits.
What About Other Stressors?
The COVID-19 pandemic is an example of a potential large-scale stressor on the WC system because it may contribute to an influx of claims involving not only physical injuries but also mental trauma. However, this is not the only potential source of escalation in mental trauma claims. Other types of events could have similar impacts at a state or local level, such as shootings, natural disasters and domestic terrorism.
Events involving mass injuries or casualties could lead to spikes in reported PTSD cases, which would present a challenge when projecting future PTSD incidence rates.
Understanding How PTSD May Affect WC System Costs
In all situations, one must account for how state law treats physical-mental, mental-physical and mental-mental events when assessing their potential impact on WC system costs.
When analyzing how proposed PTSD legislation may affect a state’s WC system, one must first consider issues related to estimating the number of compensable claims, including:
- Nuances in current and proposed WC statutes—What are the eligibility requirements, and how are they changing?
- Studies of PTSD prevalence rates—Are the prevalence rates for the lifetime or a recent period? What were the exact occupations of the participants in these studies? What DSM (American Psychiatric Association’s Diagnostic and Statistical Manual of Mental Disorders) standard was used? Did the study use clinical reporting or self-reporting? If the latter, what cutoff point of scores was used to determine the presence of PTSD? Were the participants selected at random or by convenience? What was the sample size? When was the study conducted? What country did the participants live in?
- Other factors that might cause actual claim frequency to be different than otherwise expected—Will frequency be lower due to any potential perceived stigma associated with reporting a mental injury claim? Conversely, will frequency be higher if there are financial incentives for being diagnosed with PTSD?
WC benefits available to workers with PTSD may vary significantly by state and by occupation. Considerations when estimating the average WC cost of a PTSD claim include:
- Types of medical treatment provided—Beyond the cost of counseling sessions and primary care office visits, what medicines may be prescribed to sufferers of PTSD? What health issues may arise directly related to PTSD or related to the treatment provided, such as side effects of prescription drugs? Might there be cases of self-harm?
- Temporary versus permanent disability—How might healthcare professionals determine when a worker has reached maximum medical improvement? How likely is it that a worker will be found to have a permanent total disability due to PTSD? How will benefits be determined in cases where the worker has a permanent partial disability? How will statutory time limitations affect expected costs?
See also: Addressing PTSD in the Workplace
Conclusion
Mental health conditions in the workplace are receiving greater attention, whether they arise from a single event or continual exposure to an unusually traumatic work environment. Many state legislatures have been considering establishing or expanding the eligibility for WC benefits to those suffering from work-related PTSD. And COVID-19 could intensify this trend.
To gauge the impact of PTSD claims by occupational group and on overall costs, one needs to estimate the number and average cost of such claims. Recognizing the scarcity of WC-specific PTSD claims data, a projection of the potential impact that PTSD claims may have on WC costs may result from analyzing available literature and incorporating key considerations. These considerations include the extrapolation of prevalence rates to estimate annual WC claim frequency and the applicability of historical studies to the current situation, given the locations, time periods and methodologies underlying such studies.