
Throughout this series, I have stressed the importance of connecting workers’ comp patients with great doctors at their time of need and how this results in an average of a 10% reduction in claims costs. I’ve also talked about the role of PPOs and EPOs. Next up: outcomes strategies for each jurisdiction. Workers’ compensation is determined state-by-state, requiring any national workers’ comp company to adhere to variations in the laws. Some states provide excellent control over care, while others allow so much choice that it can seem like there is no strategic use for an outcomes-based network. States use three main categories of jurisdictional control: panel (employee has to select from your list of doctors), care direction (you tell the employee who to use) and employee choice (employees choose their doctors on their own). The graphic below provides a visual breakdown of each state’s model: 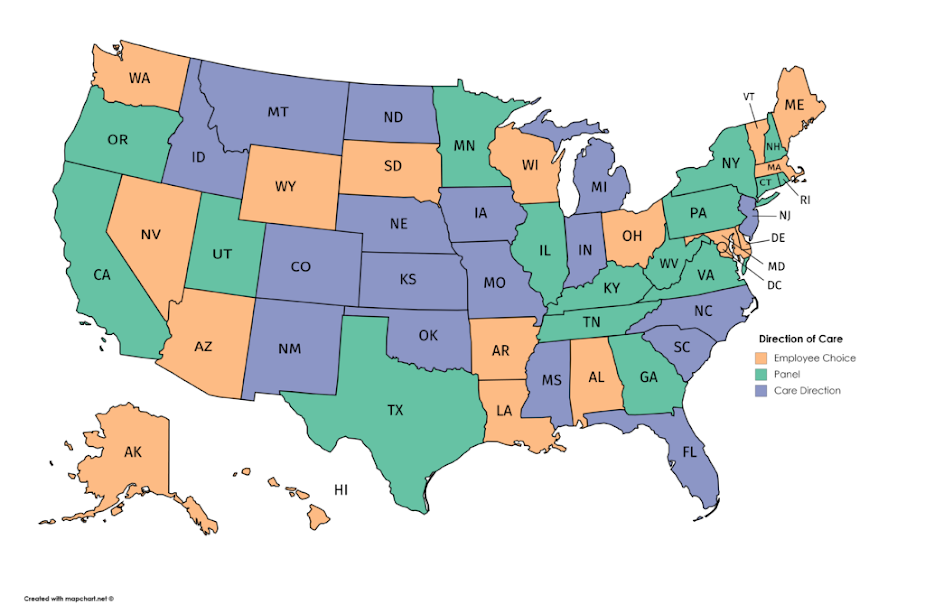 Despite what you might think, outcomes can play a meaningful role in any of these jurisdictions. Let’s discuss each model in more detail. Panel States In a panel state, employees are required to choose their doctors from a list created by payers or employers. These can range from exclusive provider networks (EPOs) to simple panels. The employee could be mandated to use doctors on the list for the life of an injury (as in the California MPN), or the designated doctor could maintain control for at least a meaningful portion of the claim (e.g., Pennsylvania workplace panels). The important consideration is that the employee can typically select anyone on your list. There is no way to manage around average doctors in your network, so it is in your best interest not to file your entire PPO as your exclusive provider listing. If you do, your overall average outcomes drop to the average across all doctors included, and you will have little recourse if injured workers choose the worst doctors on your list. For this reason, it is critical to stay on top of who’s included. Remove poor performers to ensure that any provider on that list can be trusted at any time. See also: 2018 Workers’ Comp Issues to Watch My best practice recommendation is to “right-size” your EPO by first predicting how many doctors are necessary in each coverage area (typically about a 15-mile radius). Once you know your needs for appropriate coverage, then pull only that number starting with the best and working down the ranking. The tighter you keep participation, the more impact you will see on claims outcomes. A well-constructed model can leverage provider outcome and drive overall claims costs down by 10% or more. The downside of this model is the level of effort required to maintain your list. You should keep inclusion/exclusion criteria documented up front, so you have a structured plan for whom to keep and whom to remove. You also need to check in at least quarterly to remove anyone whose performance has dropped or who has moved or closed his or her practice. Typically, you are handing over a list and letting the employee select a provider. If there is a problem (such as a provider closing the practice and not notifying you), you probably won’t realize you have an issue until you hear from the injured worker’s lawyer. Key strategic driver: Focus on the providers in your listing at all times and keep the list tight. Care Direction States In a care direction state, the insurer or payer maintains the exclusive right to tell the injured worker which doctor to use. The biggest difference over a panel model is that providers can be selected in real time. This makes maintenance a lot easier because you don’t need to “right-size” the network and anticipate needs. What you do need is an integrated view of your networks that includes your scores. In care direction states, it is critical that the search engine your team uses to direct care shows the scores of the doctors. Any time a patient needs a doctor or specialists, you want your team selecting the best available provider proximate to the injured worker — not just the closest one in network. When outcomes as a measure first matured to the point where it was widely adopted, most people focused on using outcomes to select their networks for panel states. However, the care direction model actually has a higher potential ROI because you are always selecting the best provider at the time of need. In a panel state model, when I hand over a list, the average quality of all the doctors on the list will drive the impact on your claims population. In care direction, I am always selecting the best, which drives impact to the quality of your best doctors. In addition, because the scoring updates in real time, you are always making your care decision on the latest information at the time of need, not on the information available when you built your list. Also, your best strategy is to not limit yourself to your existing network. If you are looking for a top neurosurgeon in a rural area, and there are not any good options in your PPO, you should look for a high-scoring doctor outside your network before you send the patient a longer distance to an average doctor in your PPO. As I explained earlier in the series, the outcomes savings will almost always be more than the PPO discount. Key strategic driver: Always go for the best doctors available, keeping your scores integrated with your list. Employee Choice States Many people falsely believe that outcomes-based control strategies cannot work in a state that allows the employee to select whomever they want. This is not true. Soft channeling is a strategy that involves making targeted recommendations throughout the cycle of the claim. For example, selection of the doctors that show up on the workplace poster should be based on the best doctors nearby — not just the closest. Using outcomes scores when creating workplace panels helps encourage good choices without stepping on the rights of the employee. Another strategy for the employee choice model is to integrate scores into your billing workflow. If you see an initial consult from a poor-performing ortho, you have about two weeks before your claimant goes under the knife. If you can operationalize this strategy, you have the opportunity to reach out to the injured worker with a crafted message such as: “We typically recommend a second opinion in cases like yours; there is a great specialist not far from you. Would you like me to set up an appointment?” See also: The State of Workers’ Compensation The point is to not interfere with the injured worker’s choice while taking every opportunity to provide great options for the person to consider. If your scoring model is focused on quality-of-life outcomes such as less time away from work or lower disability rates at the end of care, you are providing a valuable service to that injured worker when you steer the person away from a doctor who has high infection rates and a high incidence of failed surgeries. Certainly, the potential ROI is not as significant as in other states, but you only need a small number of injured workers to choose a better doctor to recoup typical costs of implementing these strategies. Wrapping Up There are methods and strategies to leverage outcomes in all jurisdictions. Some jurisdictions are easier than others, and your ROI and level of effort will vary, but don’t lose sight of why this is important: Better care improves everyone’s outcomes. Better outcomes improve not only the bottom line but also the quality of life for people who get injured on the job. Better care results in happier and more productive employees, fewer costly complications, less legal friction and, ultimately, a better workers’ comp system. Throughout this series of articles, I’ve covered multiple aspects of outcomes-based networks, including important considerations and strategies. These are recommendations and best practices pulled from my experiences. You don’t have to hit a home run every time. If you simply get 5% to 10% of the claims away from bad doctors and into the care of great doctors, you will have significantly better results overall. Please reach out with questions and feel free to comment with ideas for additional articles on the future of workers’ comp. As first published in Claims Journal.
Despite what you might think, outcomes can play a meaningful role in any of these jurisdictions. Let’s discuss each model in more detail. Panel States In a panel state, employees are required to choose their doctors from a list created by payers or employers. These can range from exclusive provider networks (EPOs) to simple panels. The employee could be mandated to use doctors on the list for the life of an injury (as in the California MPN), or the designated doctor could maintain control for at least a meaningful portion of the claim (e.g., Pennsylvania workplace panels). The important consideration is that the employee can typically select anyone on your list. There is no way to manage around average doctors in your network, so it is in your best interest not to file your entire PPO as your exclusive provider listing. If you do, your overall average outcomes drop to the average across all doctors included, and you will have little recourse if injured workers choose the worst doctors on your list. For this reason, it is critical to stay on top of who’s included. Remove poor performers to ensure that any provider on that list can be trusted at any time. See also: 2018 Workers’ Comp Issues to Watch My best practice recommendation is to “right-size” your EPO by first predicting how many doctors are necessary in each coverage area (typically about a 15-mile radius). Once you know your needs for appropriate coverage, then pull only that number starting with the best and working down the ranking. The tighter you keep participation, the more impact you will see on claims outcomes. A well-constructed model can leverage provider outcome and drive overall claims costs down by 10% or more. The downside of this model is the level of effort required to maintain your list. You should keep inclusion/exclusion criteria documented up front, so you have a structured plan for whom to keep and whom to remove. You also need to check in at least quarterly to remove anyone whose performance has dropped or who has moved or closed his or her practice. Typically, you are handing over a list and letting the employee select a provider. If there is a problem (such as a provider closing the practice and not notifying you), you probably won’t realize you have an issue until you hear from the injured worker’s lawyer. Key strategic driver: Focus on the providers in your listing at all times and keep the list tight. Care Direction States In a care direction state, the insurer or payer maintains the exclusive right to tell the injured worker which doctor to use. The biggest difference over a panel model is that providers can be selected in real time. This makes maintenance a lot easier because you don’t need to “right-size” the network and anticipate needs. What you do need is an integrated view of your networks that includes your scores. In care direction states, it is critical that the search engine your team uses to direct care shows the scores of the doctors. Any time a patient needs a doctor or specialists, you want your team selecting the best available provider proximate to the injured worker — not just the closest one in network. When outcomes as a measure first matured to the point where it was widely adopted, most people focused on using outcomes to select their networks for panel states. However, the care direction model actually has a higher potential ROI because you are always selecting the best provider at the time of need. In a panel state model, when I hand over a list, the average quality of all the doctors on the list will drive the impact on your claims population. In care direction, I am always selecting the best, which drives impact to the quality of your best doctors. In addition, because the scoring updates in real time, you are always making your care decision on the latest information at the time of need, not on the information available when you built your list. Also, your best strategy is to not limit yourself to your existing network. If you are looking for a top neurosurgeon in a rural area, and there are not any good options in your PPO, you should look for a high-scoring doctor outside your network before you send the patient a longer distance to an average doctor in your PPO. As I explained earlier in the series, the outcomes savings will almost always be more than the PPO discount. Key strategic driver: Always go for the best doctors available, keeping your scores integrated with your list. Employee Choice States Many people falsely believe that outcomes-based control strategies cannot work in a state that allows the employee to select whomever they want. This is not true. Soft channeling is a strategy that involves making targeted recommendations throughout the cycle of the claim. For example, selection of the doctors that show up on the workplace poster should be based on the best doctors nearby — not just the closest. Using outcomes scores when creating workplace panels helps encourage good choices without stepping on the rights of the employee. Another strategy for the employee choice model is to integrate scores into your billing workflow. If you see an initial consult from a poor-performing ortho, you have about two weeks before your claimant goes under the knife. If you can operationalize this strategy, you have the opportunity to reach out to the injured worker with a crafted message such as: “We typically recommend a second opinion in cases like yours; there is a great specialist not far from you. Would you like me to set up an appointment?” See also: The State of Workers’ Compensation The point is to not interfere with the injured worker’s choice while taking every opportunity to provide great options for the person to consider. If your scoring model is focused on quality-of-life outcomes such as less time away from work or lower disability rates at the end of care, you are providing a valuable service to that injured worker when you steer the person away from a doctor who has high infection rates and a high incidence of failed surgeries. Certainly, the potential ROI is not as significant as in other states, but you only need a small number of injured workers to choose a better doctor to recoup typical costs of implementing these strategies. Wrapping Up There are methods and strategies to leverage outcomes in all jurisdictions. Some jurisdictions are easier than others, and your ROI and level of effort will vary, but don’t lose sight of why this is important: Better care improves everyone’s outcomes. Better outcomes improve not only the bottom line but also the quality of life for people who get injured on the job. Better care results in happier and more productive employees, fewer costly complications, less legal friction and, ultimately, a better workers’ comp system. Throughout this series of articles, I’ve covered multiple aspects of outcomes-based networks, including important considerations and strategies. These are recommendations and best practices pulled from my experiences. You don’t have to hit a home run every time. If you simply get 5% to 10% of the claims away from bad doctors and into the care of great doctors, you will have significantly better results overall. Please reach out with questions and feel free to comment with ideas for additional articles on the future of workers’ comp. As first published in Claims Journal.
Why WC Needs an Outcomes Strategy
States take different approaches to choosing workers' comp doctors, but ranking based on outcomes always delivers benefits.






