

Why is it that every time I go to a doctor, I am given an appointment for a precise time, and then every single time the doctor shows up at least 20 minutes late? Does the healthcare system hate me? Do doctors not want to fix the problem? Or are they just simply incompetent?
To dig deeper into the question, we at LeanTaaS dove into the operations of more than 50 healthcare providers this past year. We looked at resource utilization profiles at three different types of clinics - cancer infusion treatment, oncology and hematology - to understand the problem and how best to solve it.
The truth is that most healthcare providers have the patient's interest at heart and are trying their level best. However, "optimal patient slotting" is a lot more complex than might appear on the surface - in fact, it is "googol-sized" in complexity. The good news is it's a problem solvable with advanced data science; the sobering news is it MUST be solved if we are to handle the incoming onslaught of an increasing, aging patient population all carrying affordable insurance over the next 20 years.
The Doctor Will Be Right With You. NOT.
There are few things I take for granted in life, and waiting to see a doctor is one of them. The average wait time for a routine visit to a physician is 24 minutes. I am sure I am not the only one who has sat in a doctor's waiting room thinking, "You said you would see me at 3:00 p.m. - why am I being called at 3:24? This happens every time; I bet you could have predicted it. So, why didn't you just ask me to come at 3:24 instead?"
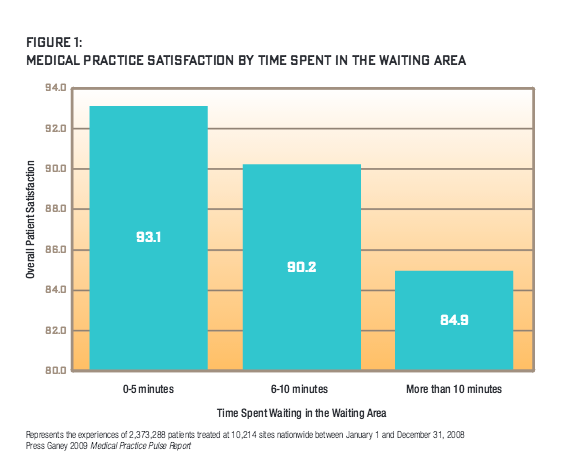
A Press Ganey study of 2.3 million patients at 10,000 sites nationwide found that a five-minute wait can drop patient satisfaction by 5%, a 10-minute wait by 10% and more than 10 minutes by 20%.
That 24-minute stat is, in fact, not so bad compared with anyone who has had to get an infusion (chemo) treatment, visit a diabetes clinic, prepare for surgery or see just about any specialist. Those wait times can be hours.
Just visit any hospital or infusion center waiting room, and you will see the line of patients who have brought books, games and loved ones along to pass that agonizing wait time before the doctor sees them.
I spent the past year researching this problem and saw for myself just how overworked and harried nurses and doctors operating across the healthcare system are. I spoke to several nurses who have had days they were not able to take a single bathroom break. Clinics routinely keep a "missed meal metric" - how often nurses miss lunch breaks - and most of the ones I spoke to ring that bell loudly every day. I even heard of stories of nurses suing hospitals for having to go a whole day without breaks or meals.
The fact is that long patient wait times are terrible for hospitals, too. Long wait times are symptomatic of chronically inefficient "patient flow" through the system, and that has serious negative impact on the hospital's economic bottom line and social responsibility:
- Lower Access and Revenue: A natural corollary to long patient wait times is that the hospital sees fewer patients than it possibly could each day. The Medical Group Management Association found that the average utilization of operating rooms at large hospitals in 2013 was only 53%. Fewer patients served directly implies reduced access to care, lower revenues and higher unit costs.
- Rising Labor Costs and Declining Nurse Satisfaction: Nurses are an expensive and scarce skill set. Because of the "peaks and valleys" caused by inefficient scheduling during the day, hospitals have to staff for the "peak" and simultaneously experience periods of low activity while still needing significant overtime hours from nurses.
Hospital leaders know this well. Every administrator I spoke to in my research - CEO / CAO / CNO - has some kind of transformation effort going on internally to improve patient flow - "lean" teams, 6-sigma teams, rules for how to schedule patients when they call into various clinics and so on. Leaders know that if patients could be scheduled perfectly and doctors could see them on time, the resulting "smoothing of patient flow" throughout the system would make their facilities, staff and the bottom line much better off.
The Real Reason
It's not for a lack of motivation that the system is broken. It's just a complex math problem.
The system is broken because hospitals are using a calculator, standard electronic health record (EHR) templates and a whiteboard to solve a math problem that needs a cluster of servers and data scientists to crunch.
To illustrate why scheduling is such a complex problem, let's take the case of a mid-sized infusion (chemo) treatment center I studied during my research.
This infusion center has 33 chairs and sees approximately 70 patients a day. Infusion treatments come in different lengths (e.g., 1-2 hours, 3-4 hours and 5-plus hours long), and the typical daily mix of patients for these three types are 35 patients, 25 patients and 10 patients, respectively. The center schedules patients every 15 minutes starting at 8:00 a.m. with the last appointment offered at 5:30 p.m. So there are 39 possible starting times: 8:00 a.m., 8:15 a.m., 8:30 a.m., etc, ending at 5:30 p.m. The center can accommodate three simultaneous starts because of the nursing workload of getting a patient situated, the IV connected, etc. That makes a total of 39*3 = 117 potential "appointment start slots."
That may not seem like a lot, but it results in 2.6 times 10 to the 61st power possible ways to schedule a typical, 70-patient day. (I'll save you the math.) That's 26 million million million million million million million million million million possibilities.
And that number is just the start. Now add in the reality of a hospital - some days nurse schedules are different from others, the pattern of demand for infusion services varies widely by day of week, doctors' schedules are uneven across the week, special occurrences like clinical trials or changes in staff need to be considered and so on. You are looking at a problem that you can't solve with simple heuristics and rules of thumb.
How Today's "Patient-Centric" Scheduling Often Works - and Backfires
Very few hospitals I spoke to understand or consider this math. Rather, in trying to "make the patient happy," most providers have been trained to use a "first come, first served" approach to booking appointments. Sometimes, providers use rules of thumb based on their knowledge of busy times of day or week, e.g., start long appointments in the morning and shorter ones later.
If hospitals were scheduling patients for one chair, one nurse and the same treatment type, some simple rules could work. But reality is a lot more complicated - the right schedule would need to consider varying treatment times across patients, include multiple treatment rooms/chairs, varying staff schedules, lab result availability and so on. Without sophisticated tools, there is an almost zero chance a scheduler can arrange appointments so treatment durations fall like Tetris blocks that align perfectly over the course of the day, and seamlessly absorb patients as they arrive, orchestrating doctor, nurse and room availability, while accounting for all the other constraints of the operation.
In effect, hospitals are scheduling "blind," not taking into account the effect of appointments already scheduled before, during or soon after the slot being allotted on a first-come basis. Schedule currently is like adding traffic to rush hour and almost always results in a "triangle shaped utilization curve" - massive peaks in the middle of the day and low utilization on either side.
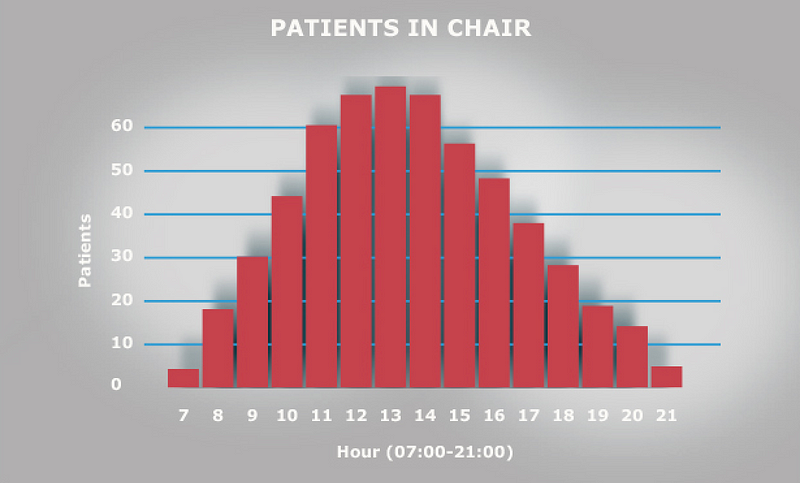
Each of the 50 hospitals I spoke to identified precisely with this utilization curve. In fact, they identify with "the midday rush and slower mornings and evenings" so well that they have given them affectionate names - one called it their "Mount Everest," another "Mount Rainier."
From a cancer center's standpoint, this chair utilization curve has several issues even beyond long patient wait times:
- The center can only see a fraction of patients it could have with a "flatter" utilization curve.
- Nurse scheduling has to be done for the peak, and the treatment center typically deals with lots of overtime issues.
- Nurses find it hard to take lunch breaks because of the midday peak, while half the time the chairs are empty.
- On any day, given the number of interdependent moving parts, a small perturbation to the system (e.g., a patient's labs are late, another patient didn't arrive on time) creates a domino effect, further exacerbating delays, not unlike a fender bender in rush hour traffic that delays everyone for hours.
In effect, when hospitals think they are scheduling in patient-centric ways, they are doing exactly the opposite.
They are promising patients what they cannot deliver - instead of giving the patient that 10:00 a.m. Wednesday appointment, an 11:40 a.m. appointment may have been much better for the patient and the whole system.
As we will see, the patient could have had a 70% shorter wait time, the hospital could have seen 20% more patients that week, every nurse could have taken a lunch break every day and a lot less (if any) overtime would have been required.
So How Do You Solve This "Googol-Sized Patient Slotting" Problem?
The solution lies in data science and mathematics, using inspiration from lean manufacturing practices pioneered by Toyota decades ago, such as push-pull models, production leveling, reducing waste and just-in-time production.
In mathematical terms, it means taking those 10^61 possibilities and imposing the right set of "constraints" - demand patterns, staffing schedules, desired breaks and whatever is unique to the hospital's specific situation - to come up with a much tighter set of possible patient arrangements that solve for maximizing the utilization of hospital resources and therefore the number of patients seen.
In the case of the infusion center, the algorithm optimizes utilization of infusion chairs, making sure they are occupied uniformly for as much of the day as possible as opposed to the "peaks and valleys" in Figure 3. In essence, "rearranging the way the Tetris blocks (patients) come in" so they appear in the exact order they can be met by a nurse, prepped and readied for a doctor whose schedule has been incorporated into the algorithm.
The first step in doing this is mining the pattern of prior appointments to develop a realistic estimate of the volume and mix of appointment types for each day of the week.
The second step is imposing the real operational constraints in the clinic (e.g., the hours of operation, doctor and nurse schedules, the number of chairs, various "rules" that depend on clinic schedules, as well as patient-centric policies such as that treatments longer than four hours should be assigned to a bed and not a chair).
Finally, constraint-based optimization techniques can be applied to create an optimal pattern of "slots," which reflect the number of "appointment starts" of each duration.
In the case of the infusion center, that means how many one-hour duration, three-hour duration and five-hour duration slots can be made available at each appointment time (i.e. 7:00 a,m., 7:15 a.m., 7:30 a.m. and so on).
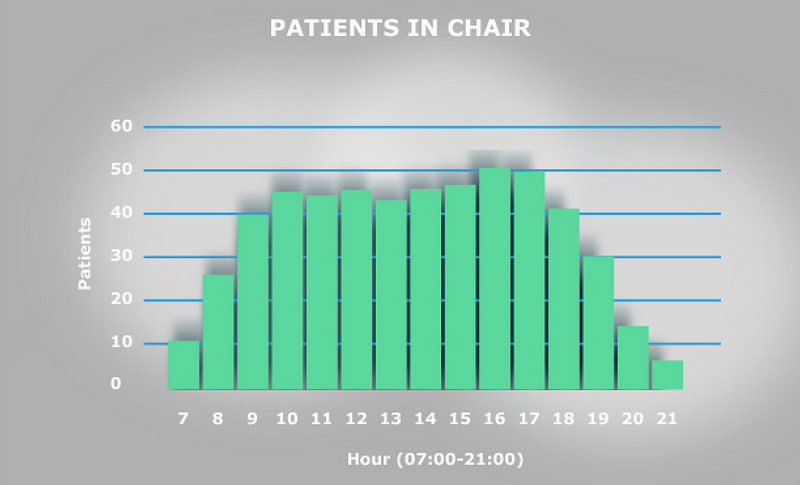
Doing this optimally results in moving the chair utilization graph from the "triangle that peaks somewhere between 11:00 a.m. and 2:00 p.m." in Figure 3 to a "trapezoid that ramps up smoothly between 7:00 a.m. and 9:00 a.m., stays flat from 9:00 a.m. until 4:00 p.m. and then ramps down smoothly from 4:00 p.m. on" in Figure 4.
Coming up with realistic slots that keep patients moving smoothly throughout the day cuts patient waiting times drastically, reduces nurse overtime without eliminating breaks and keeps chair utilization as high as possible for as long as possible. Small perturbations in this system are more like a fender bender at midnight, a small annoyance that causes a few minutes of delay for a small number of people instead of holding up rush hour traffic for hours.
Smoothing Patient Flow - A Large Economic Opportunity
The above graphs are sanitized versions of real data from a cancer infusion treatment center at a real hospital that used these techniques to solve their flow problems. The results they achieved are staggering and point to the massive economic and social opportunity optimal patient flow presents.
Post implementation of a product called "LeanTaaS iQueue," they now experience:
- 25% higher patient volumes
- 17% lower unit cost of service delivery
- 31% decrease in median patient wait times
- 50% lower nurse overtime
- Significantly higher nurse satisfaction - no missed meals
Imagine applying this kind of performance improvement to every clinic, hospital and surgery suite in the country and the impact it will have on population health through increased patient access to the system.
The Problem Is Going to Get a Lot Worse Unless Providers Address It Now
This problem is going to get a lot worse for a simple reason - the demand for medical services has never been stronger, and it's only going to increase. Just looking at the U.S. market:
- Population Growth: By 2050, there will be more than 438 million Americans, up from 320 million in 2015.
- Demographics: By 2030, more than 20% of the country is expected to be older than 65, up from 15% in 2015 - increasing the demand for chronic clinical therapies. In raw numbers, the Census Bureau estimates that by 2030, when the last round of Baby Boomers will hit retirement age, the number of Americans older than 65 will hit 71 million, up from 41 million in 2011, a 73% increase. When this happens, one in five Americans will be older than 65. Not surprisingly, by 2025, 49% of Americans will be affected by a chronic disease and need corresponding therapies.

- The Affordable Care Act: The Affordable Care Act will add 30 million Americans to the healthcare system by 2025. That means more demand for healthcare - more doctor visits, more hospital visits, more emergency emergency room visits and more need for resources (e.g., surgery rooms, MRI / CAT scans). Reimbursements will increasingly depend on outcomes and efficacy, quality of care and patient access. Unless providers become a lot more efficient in how they process and treat patients, they will need to spend billions in capital spending on new infrastructure - clinics, operating rooms, infusion centers and the like.
- In an online poll conducted by the American College of Emergency Physicians (ACEP), 86% expect emergency visits to increase over the next three years. More than three-fourths (77%) say their ERs are not adequately prepared for significant increases.
- The Commonwealth Fund, a New York-based fund that tracks healthcare performance, projects that primary care providers will see, on average, 1.34 additional office visits per week, accounting for a 3.8% increase in visits nationally. Hospital outpatient departments will see, on average, 1.2 to 11 additional visits per week, or an average increase of about 2.6% nationally.
- It is estimated that the U.S. will face a shortage of 90,000 physicians and 500,000 nurses by 2030.
The Good News
Most healthcare providers are waking up to the fact that their operations need a data-driven, scientific overhaul much the same way as auto manufacturing, semiconductor manufacturing and all other asset-intensive, "flow"-based systems have experienced.
The good news is that there are tools, software and resources that can be used to bring about this transformation. Companies like LeanTaaS are at the forefront of this thinking and are applying complex data science algorithms to help hospitals solve these problems.
Hospitals that are serious about solving patient flow issues and the related problems now have access to the best computational minds and tools.
I see a world in which our healthcare system can see every patient on time without imposing hardship on care providers, disruption on current processes or increasing cost of services.
Here's to that world!


